Axio Recovery
Cornell DEBUT · Cornell University · 8-Person Team (Project Manager)
I led an 8-person Cornell DEBUT team from blank schematic to validated diagnostic hardware, a wearable that estimates elbow torque to 2.58% error against motion-capture ground truth.
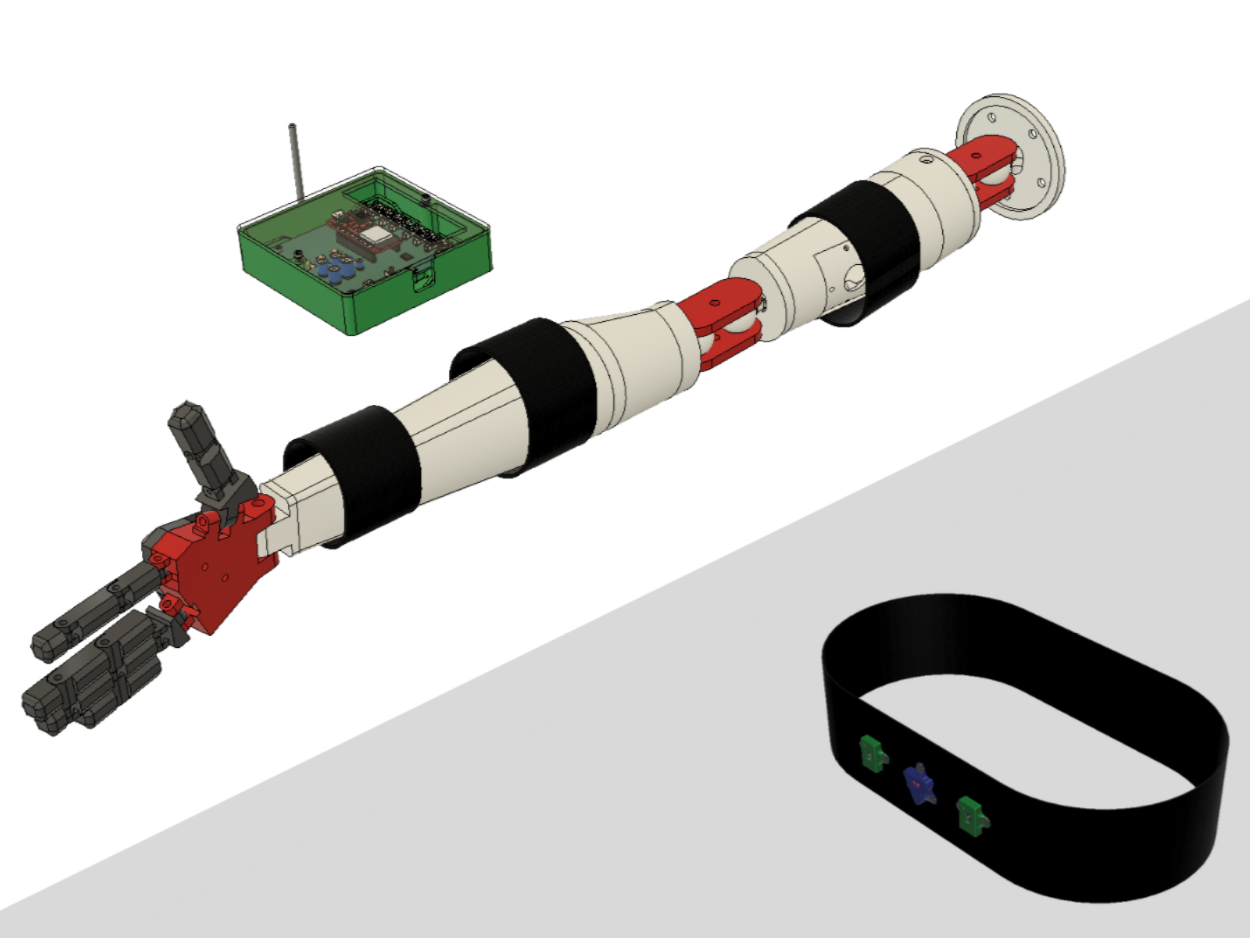
 Final system, V2.0
Final system, V2.0
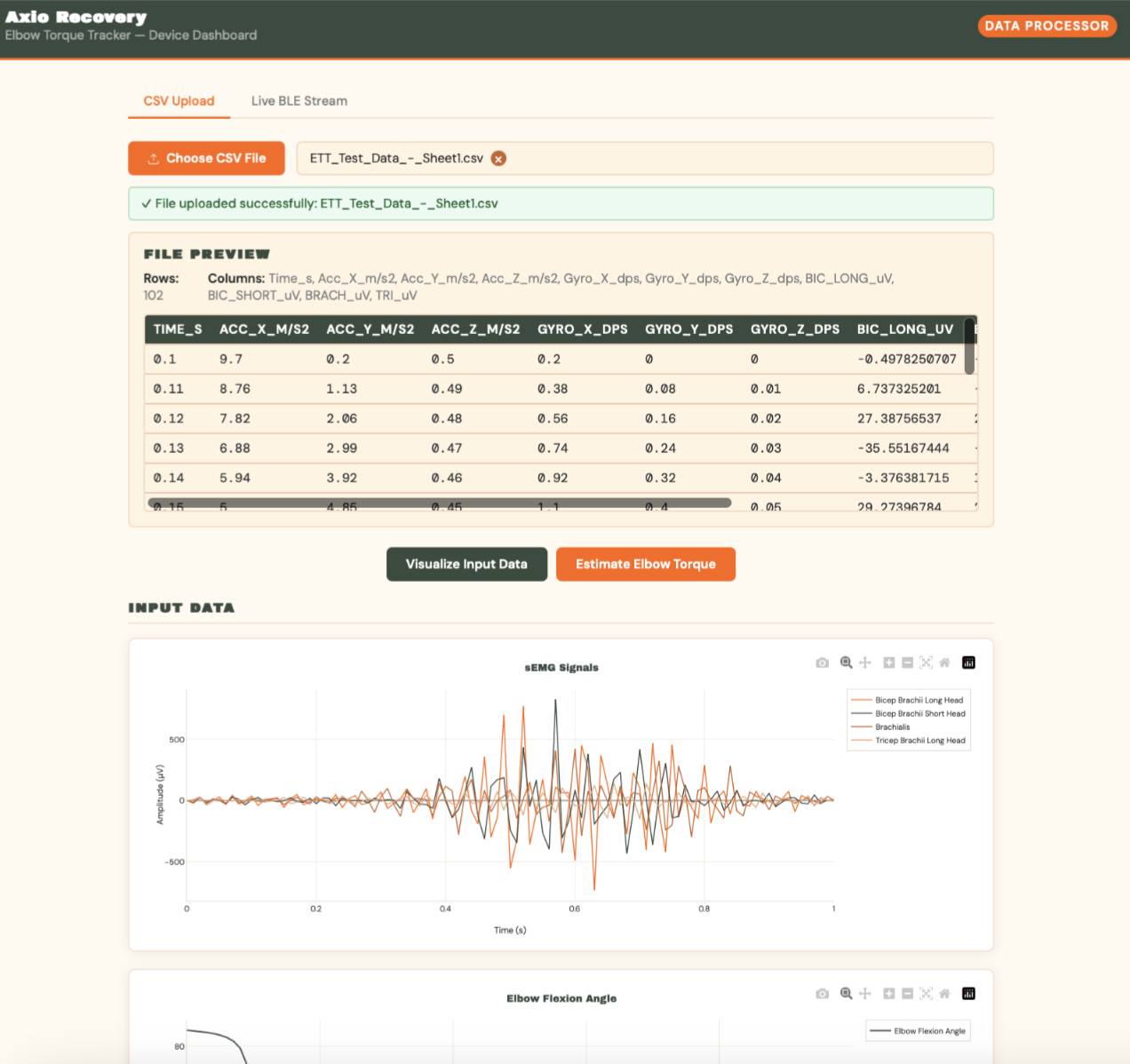 Clinician dashboard: axiorecoverytracker.com
Clinician dashboard: axiorecoverytracker.com
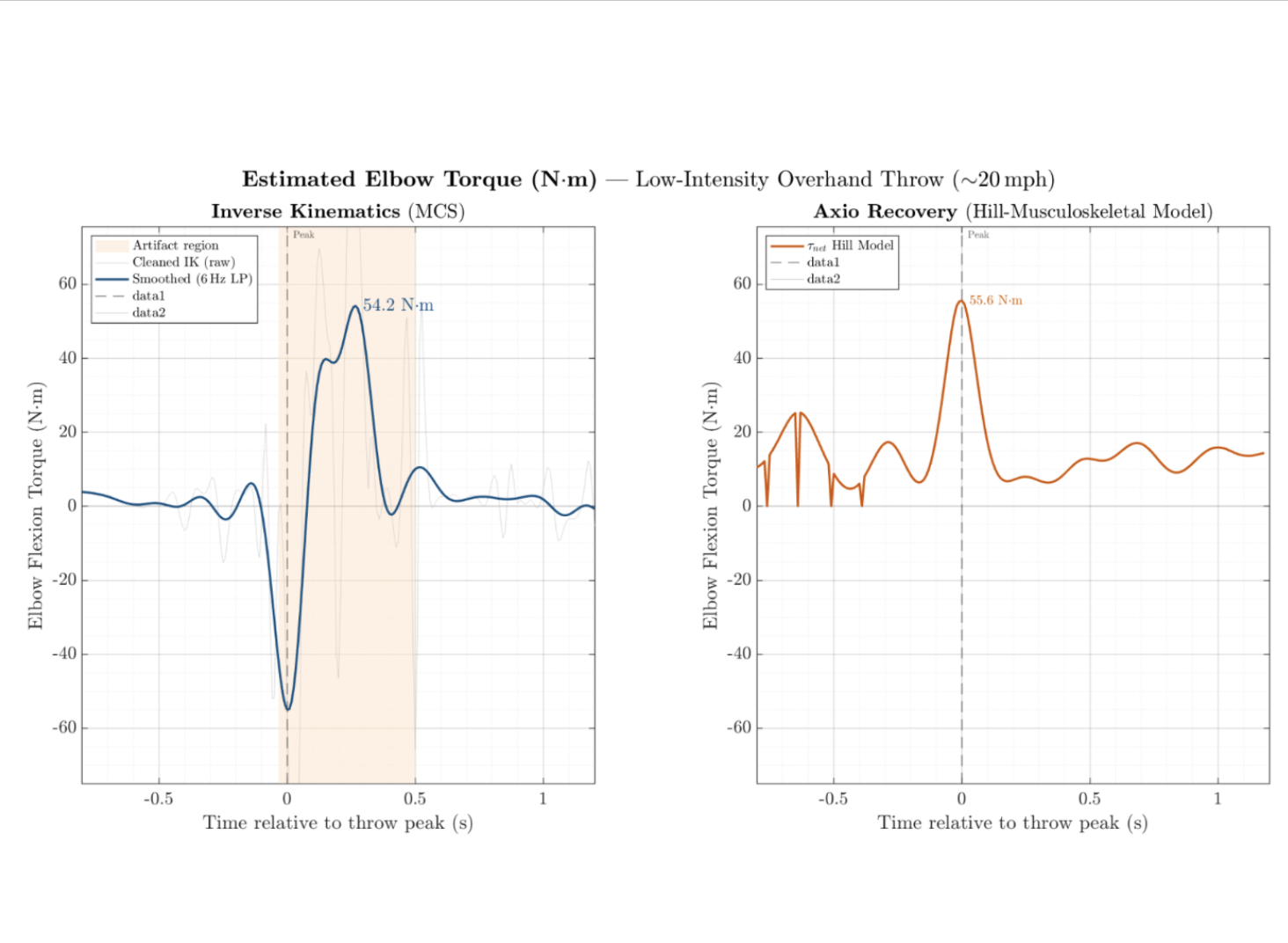 Validation: OptiTrack vs. Axio Recovery
Validation: OptiTrack vs. Axio Recovery
 Field testing: throwing motion capture
Field testing: throwing motion capture
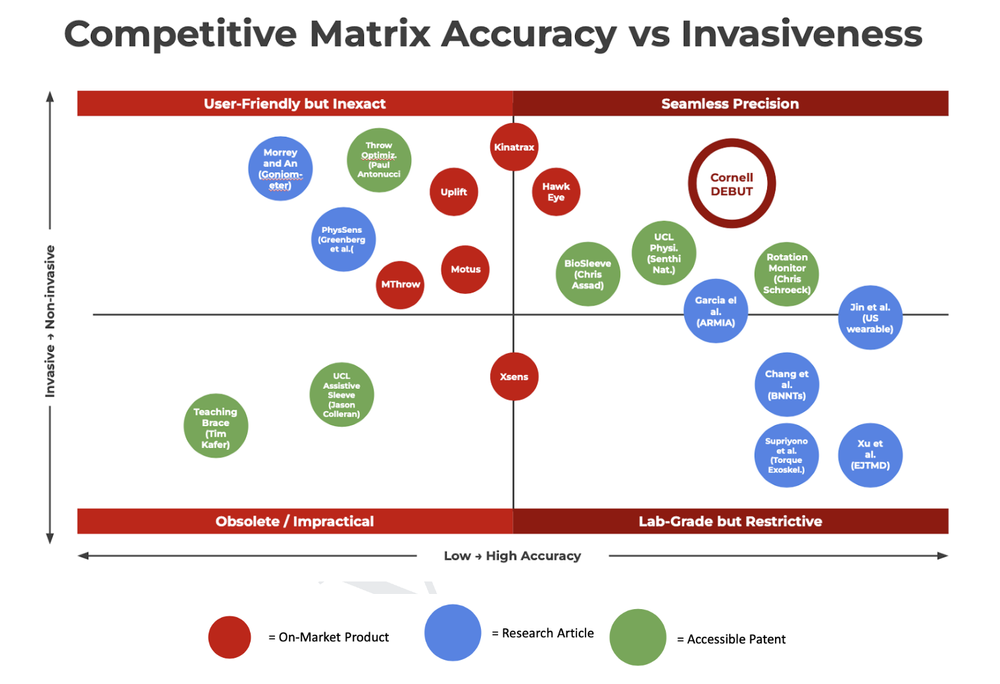 Competitive matrix: accuracy and cost targets vs. Pulse and lab motion capture
Competitive matrix: accuracy and cost targets vs. Pulse and lab motion capture
Systems Engineering
sEMG / IMU Sensing
Hill's Musculoskeletal Model
PCB Design (KiCAD)
Embedded C++
Python Signal Pipeline
Fusion360
V&V Testing
OptiTrack Motion Capture
GitLab CI
Technical Leadership